



Абстракт
В статье представлена информация об исследовании роли врожденных пороков сердца как фактора риска развития заболевания у недоношенных детей с подозрением на некротический энтероколит (НЭК). В исследование были включены 88 детей обоих полов с подозрением на НЭК. В качестве контрольной группы были взяты 30 условно здоровых недоношенных детей. Из 88 детей с подозрением на НЭК 43 были девочками и 45 — мальчиками; в контрольной группе 15 детей были девочками и 15 — мальчиками. Была изучена взаимосвязь между развитием некротизирующего энтероколита и пороками сердца, такими как открытый артериальный проток (ОАП), трикуспидальная недостаточность и открытое овальное отверстие. Исследование показало, что пороки сердца не играют роли фактора риска развития заболевания у недоношенных детей с подозрением на некротизирующий энтероколит. Таким образом, на основании результатов исследования можно сказать, что пороки сердца не играют роли фактора риска в диагностике заболевания у недоношенных детей с подозрением на некротизирующий энтероколит.
Сопроводительное письмо
İNTRODUCTİON Necrotizing enterocolitis (NEC) in newborns is an acute multifactorial disease characterized by intestinal necrosis and is one of the leading causes of morbidity and mortality in premature infants .Due to the incomplete understanding of the pathogenesis of the disease, there is a lack of effective and reliable methods for the prevention and treatment of the disease. Identification of newborns suspected of having NEC and early intervention in them may play a crucial role in reducing the incidence of the disease and improving the prognosis [1].
For this purpose, a number of risk factors leading to the disease have been identified, and newborns with congenital heart defects are included in the high-risk group [2]. Among heart defects, especially PDA (patent ductus arteriosus) is an important risk factor for NEC. Congenital heart defects (including PDA) cause inadequate blood flow distribution, trigger an immune response, stimulate inflammatory mediators, and cause damage and necrosis of the intestinal mucosa, ultimately leading to necrotizing enterocolitis [3]. According to recent literature data, the mortality rate of NEC in children with congenital heart defects is high, reaching 25% [4]. Considering all this, we found it important to study risk factors in our study in order to improve early diagnosis of the disease in premature infants with suspected NEC.
The above-mentioned confirms the relevance of the current study and creates a basis for conducting research in this aspect. The aim of the study: To determine the role of congenital heart defects in the development and progression of the disease in premature infants with suspected signs of necrotizing enterocolitis.
MATERİALS AND METHODS The study is based on the results obtained from studying the role of congenital heart defects in the development of the disease in premature infants with initial suspicion of NEC. The study was conducted at the Scientific Research Institute of Pediatrics named after K.Y. Farajova, Republican Perinatal Center, Baku Medical Plaza, Maternity Hospital No. 5 named after Sh. Alasgarova (2020-2023). 88 prematurely born children were involved in the study. Of these, 43 were girls and 45 were boys. Mean gestational age - 31.03±2.68 weeks (mean±SD), median 31.50 weeks; (minimum 26 weeks, maximum 36 weeks); mean weight 1478.3±464.35 (mean±SD); median 1440.00; minimum 800g, maximum 2500g. Of these children, 29 (32.5%) were confirmed with NEC diagnosis, while in 59 (67.1%) the diagnosis were denied. The mean gestational age of children with confirmed NEC 31,17±3,07 weeks (Mean±SD), mean weight 1590,34±534g (Mean±SD), the children with denied diagnosis of desease the mean gestational age was 31±2,50 weeks (Mean±SD), body weight 1423,3±420g. The diagnosis of NEC was confirmed based on clinical, laboratory and instrumental indicators. In all patients, abdominal distension, feeding intolerance, vomiting, (mainly with bile), blood in the stool, apnea, etc. were taken as the initial clinical signs of NEC. Exclusion criteria from the study:
- congenital and chromosomal anomalies;
- infants without suspicion of NEC during the first 3 weeks.
The Chi-Square (X2) test was used to compare categorical variables obtained from the study, and p<0.05 reflected the statistical significance of the difference. Statistical processing of the indicators was carried out in the Windows SPSS20 system. The arithmetic mean (based on all the quantitative indicators we received - mean (average indicator); SD - how much the indicators differ from the mean square difference) and the minimum and maximum indicators were given.
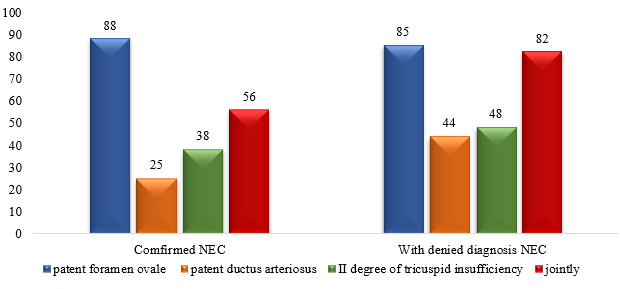
RESULTS AND DİSCUSSİON There are several studies that indicate that there is a direct relationship between the persistence of fetal blood circulation in the early neonatal period in premature infants, the development of necrotizing enterocolitis in cases where the foramen ovale and the patent ductus arteriosus remain open [5, 6].
In our study, no such relationship was noted between the presence of patent ductus arteriosus and the confirmation of the diagnosis of NEC. According to several literature data, no statistically significant relationship was noted between congenital heart pathologies and NEC [7]. Also, since the most common pathology found during echocardiography examination is II degree of tricuspid regurgitation, we tried to study the significance of this pathology in the confirmation of the diagnosis of NEC, and it was found that this degree of tricuspid regurgitation was also statistically insignificant in the confirmation of the diagnosis of NEC.
Thus, as can be seen from this study, we did not find an association between congenital heart defects and the development of necrotizing enterocolitis in our study. Congenital heart defects, by impairing mesenteric perfusion, lead to prolonged hospitalization and increased risk of death in children with NEC [8]. Therefore, their investigation as a risk factor in patients with suspected NEC is important and vital.
Фигуры
Ключевые слова
Ссылки
1.Su Y., Xu R.H., Guo L.Y. et al. Risk factors for necrotizing enterocolitis in neonates: A meta-analysis // Frontiers in pediatrics, 2023, Jan 6; (10): 1079894. doi:10.3389/fped.2022.1079894.
2.Kashif H., Abuelgasim E., Hussain N. et al. Necrotizing enterocolitis and congenital heart disease // Annals of pediatric cardiology, 2021, 14 (4): 507–515. https://doi.org/10.4103/apc.apc_30_21
3.Zhao S., Jiang H., Miao Y. et al. Factors influencing necrotizing enterocolitis in premature infants in China: a systematic review and meta-analysis // BMC Pediatrics, 2024, 24 (1): 148. doi:10.1186/s12887-024-04607-3
4.Schramm, J., Bhargava, C., Cedric M. et al. 884: Rısk factors for necrotızıng enterocolıtıs ın congenıtal heart dısease usıng machıne learnıng // Critical Care Medicine, 2025, 53(1). DOI: 10.1097/01.ccm.0001102200.99649.43
5.Kelleher S.T., McMahon C.J., James A. Necrotizing Enterocolitis in Children with Congenital Heart Disease: A Literature Review // Pediatric Cardiology, 2021, 42 (8): 1688-1699. doi: 10.1007/s00246-021-02691-1.
6.Campos-Martinez A.M., Expósito-Herrera J., Gonzalez-Bolívar M. et al. Evaluation of Risk and Preventive Factors for Necrotizing Enterocolitis in Premature Newborns. A Systematic Review of the Literature // Frontiers in Pediatrics, 2022, 10:874976. doi:10.3389/fped.2022.874976
7.Çakmak H.M., Kocabay K. Risk Factors of Necrotizing Enterocolitis in Preterm Infants: A Single Center Experience / Haydarpaşa Numune Medical Journal, 2024, Volume: 64, Number: 2, Page: 187-192. DOI: 10.14744/hnhj.2023.74555
8.Kaplina A., Kononova S., Zaikova E. et al. Necrotizing Enterocolitis: The Role of Hypoxia, Gut Microbiome, and Microbial Metabolites / İnternational journal of molecular sciences, 2023, Jan 27; 24(3):2471. doi: 10.3390/ijms24032471.
О статье:
История публикации
Опубликовано: 14.May.2026
Авторское право
© 2022-2025. Azerbaijan Medical University. E-Journal is published by "Uptodate in Medicine" health sciences publishing. All rights reserved.Связанные статьи
Просмотрено: 704